Sleep apnea isn't one single thing. Most people treat it that way. But there are different types, they happen for different reasons, and they don't respond to the same treatment.
That distinction matters more than people realise. Getting the type wrong means the treatment won't work. Sometimes it makes things worse.
The One Thing Both Types Share
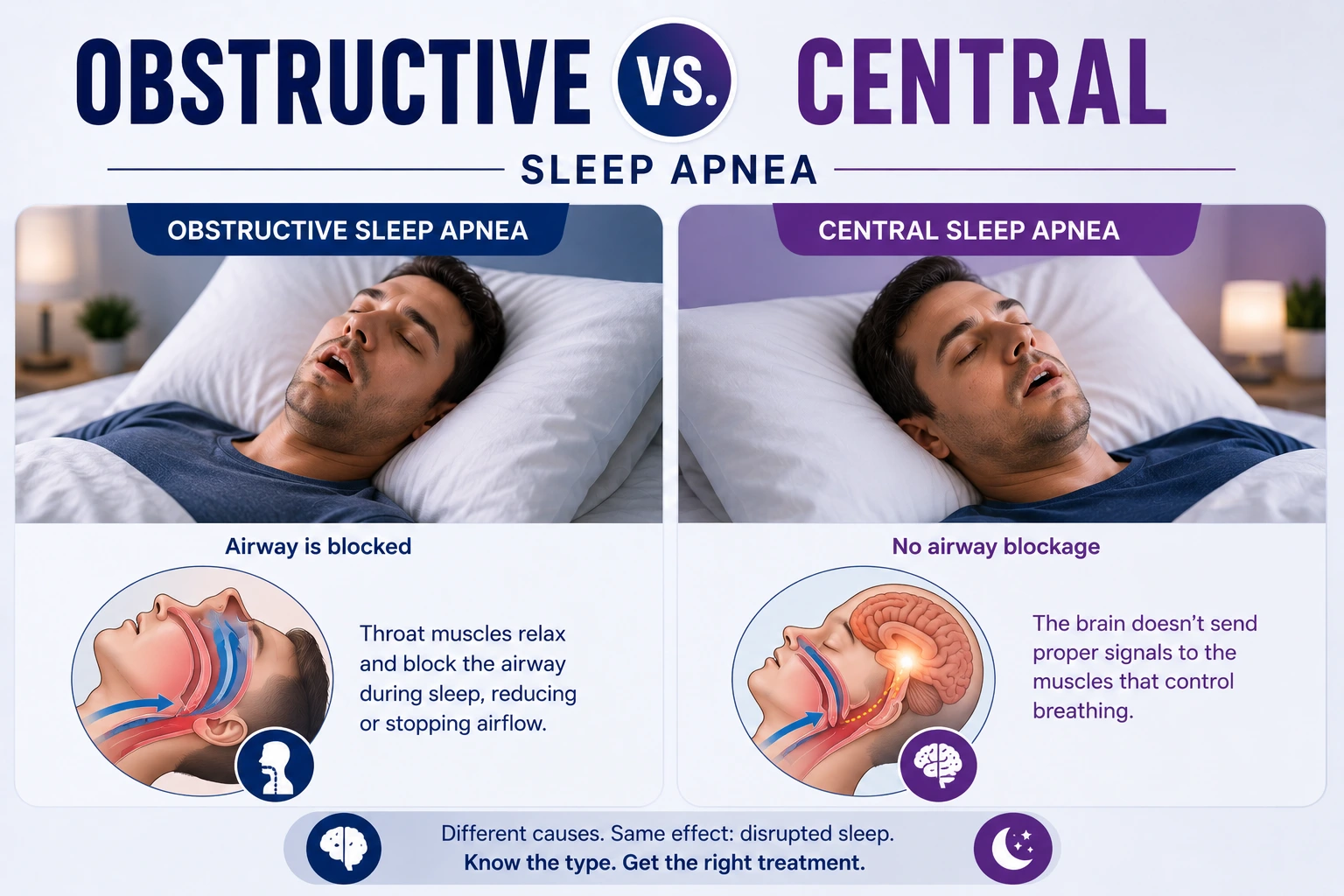
In both obstructive and central sleep apnea, breathing stops during sleep. These pauses reduce oxygen in the blood. They break up sleep. They cause brief awakenings the person rarely remembers.
The result feels the same either way. You wake up exhausted. You drag through the day. Morning headaches are common. Concentration is hard. Mood takes a hit.
From the outside, the two types can look almost identical. What differs is why the breathing stops.
Obstructive Sleep Apnea: When the Airway Collapses
OSA is by far the more common type. It accounts for the vast majority of sleep apnea cases.
The problem is physical. The airway narrows or closes during sleep — not because of anything the person does consciously, but because the muscles holding the throat open relax too much.
When we fall asleep, muscles throughout the body relax. That includes the throat. In most people, the airway stays open enough for breathing to carry on. But in people with OSA, those tissues relax further. The soft palate, the tongue base, the walls of the throat come together. Air forces its way through. That's what causes snoring. Sometimes the airway closes almost fully. Breathing stops.
The brain detects the drop in oxygen. It briefly rouses the body. Just enough to restore muscle tone and reopen the airway. A gasp, a snort, a shift in position. Then sleep resumes.
Then it happens again.
This can occur five times an hour in mild cases. Sixty or more in severe ones. Most patients have no memory of it. They just know they woke up tired. Again.
What Makes the Airway More Likely to Block?
Some people have naturally narrower airways. A jaw that sits further back. A larger tongue. Excess soft tissue at the back of the throat. These features reduce available space and make collapse more likely during sleep.
Weight is one of the strongest risk factors. Fat tissue around the neck puts pressure on the airway from outside. The heavier that load, the easier it closes. This is why OSA often builds slowly, quietly tracking alongside weight changes over years.
Age plays a role too. Muscle tone reduces with time, including in the throat. Sleeping on the back lets the tongue fall backward more easily. Alcohol relaxes muscles further. Many patients notice their symptoms are worse after drinking in the evening.
It often develops slowly. People don't always connect the dots early.
Central Sleep Apnea: When the Brain Stops Sending the Signal
Central sleep apnea (CSA) is less common. But it's often more complex to manage.
The mechanics are completely different. The airway is clear. There's no physical blockage, no collapsing tissue. The throat is open. The problem is that the brain simply doesn't send the signal to breathe.
Breathing during sleep should be automatic. The brainstem monitors carbon dioxide in the blood and tells the breathing muscles to contract. Inhale. Exhale. Repeat. No conscious effort needed.
In CSA, that system misfires. The signal doesn't arrive reliably. The breathing muscles sit idle. And breathing stops.
There's no snoring during these episodes. No snort as the airway reopens. Just silence. That's part of why it can be harder for a bed partner to notice — the pattern simply looks different from the obstructive type.
What Causes Central Sleep Apnea?
Unlike OSA, CSA is usually tied to other medical conditions.
Heart failure is one of the most common links. When the heart isn't pumping well, the body's handling of carbon dioxide and oxygen becomes unstable. The feedback loop controlling breathing breaks down. A specific pattern called Cheyne-Stokes respiration can develop — breathing gradually increases, then decreases, then pauses, then starts again in a repeating cycle. It's a form of CSA seen in people with significant heart failure.
Stroke and some brain conditions can also disrupt the pathways that control breathing at night. The automatic regulation of breathing becomes unreliable.
Strong opioid pain medications are another cause. They suppress the brain's drive to breathe. At night, when the body is already less alert, that suppression can trigger repeated central pauses.
High altitude is a less common cause but a recognised one. Lower oxygen in the air creates an unstable breathing cycle. Most people descend before it becomes a clinical problem.
Some patients also develop CSA after starting CPAP therapy for OSA. The obstructive episodes are resolved, but central events appear. This is called treatment-emergent central sleep apnea. It often settles over time with monitoring, but sometimes a change in the treatment device is needed.
Mixed Sleep Apnea: When It's Both
Some patients have a mix of obstructive and central events. The same night can include both. Or the pattern shifts as treatment progresses.
This is sometimes called mixed or complex sleep apnea. Both mechanisms are contributing, so treatment has to address both. That usually means a more advanced device than standard CPAP.
Mixed apnea is more common than people expect. It's one reason a proper sleep study matters before any treatment decision is made.
Why the Type Changes Everything About Treatment
Standard CPAP delivers steady pressurised air through a mask during sleep. It holds the airway open from the inside. For obstructive sleep apnea, that works well. The physical collapse is prevented. Breathing stays steady. Oxygen stays stable.
But for CSA, the airway isn't the problem. It's already open. Pushing air through a clear airway doesn't fix a brain signalling issue. In some cases, standard CPAP can actually worsen central events by disturbing the carbon dioxide balance the brainstem relies on.
CSA often needs a different device entirely.
BiPAP delivers different pressures for breathing in versus breathing out. Some patients tolerate it better than CPAP. Adaptive servo-ventilation is more complex. It monitors breathing in real time and adjusts automatically, effectively backing up breathing when the brain's signal drops. ASV is particularly useful for the Cheyne-Stokes pattern seen in heart failure patients.
But ASV isn't right for everyone. There are specific cases where it shouldn't be used, including certain types of heart failure. The most advanced device isn't always the right one.
For CSA caused by medications, reviewing those medications is part of the plan. For cases tied to heart failure, managing the heart condition directly sits at the centre of treatment, not alongside it.
Obstructive sleep apnea has its own treatment range beyond CPAPoral devices for milder cases, positional changes, weight management, surgical options for specific structural problems. None of those touch central events.
Getting the type wrong leads to treatments that don't land. That's why the distinction matters in practice, not just on paper.
You Can't Tell the Difference Without a Sleep Study
Patients often ask if they can figure out which type they have from symptoms alone. They can't. And neither can a doctor without testing.
Both types produce the same daytime picture. Fatigue. Poor focus. Mood changes. Morning headaches. Sleep that never feels restorative.
Loud snoring and the classic choking pattern are more associated with OSA. CSA tends to be quieter. But these are tendencies, not reliable rules. Some people with obstructive sleep apnea don't snore noticeably. Some with CSA do make sounds as breathing restarts.
The only way to tell them apart is a sleep study that measures both airflow and breathing effort at the same time.
Airflow tells us when breathing stops. Breathing effort tells us whether the body was still trying during that pause.
Effort present, airflow blocked: obstructive.
No effort at all: central.
Effort starts partway through the pause: often mixed.
A basic pulse oximeter can't make this distinction. A snoring app can't either. The monitoring has to be specific to capture it.
What Assessment Looks Like
When patients come to Dr. Syed Arshad Husain at Al Zahra Hospital in Dubai with symptoms suggesting sleep apnea, the assessment is thorough.
The consultation covers the full symptom history. When tiredness started. What sleep quality has been like. Whether a bed partner has noticed anything. Daytime functioning, mood, concentration. Medical history is reviewed in detail too: heart conditions, any history of stroke or brain injury, current medications, weight changes, thyroid conditions, and relevant hormonal factors.
For patients with heart failure or those on regular opioid medications, CSA is considered from the start. The clinical picture shapes what type of sleep study is arranged and what the results need to focus on.
The sleep study itself is most often done at home. It records airflow, breathing effort, oxygen levels, heart rate, and sleep position through the night. Results are reviewed in detail before any treatment decision is made.
Diagnosis drives the plan. Not a generic approach. One matched to the type, the causes, the severity, and the individual patient.
What Recovery Looks Like
For obstructive sleep apnea with the right device at the right settings, improvement can come quickly. Some patients feel a difference within the first week. Energy lifts. Brain fog clears. Mornings feel different.
For CSA, recovery depends more on the underlying cause. When heart failure is the driver, managing the heart condition alongside sleep treatment can make a real difference. When medications are involved, adjustments take time.
Treatment-emergent central events after starting CPAP often settle over weeks with close monitoring. Mixed apnea needs more follow-up checking the device is handling both components, adjusting settings as needed.
Follow-up isn't optional here. Repeat studies are sometimes needed to confirm treatment is working. Device data is reviewed. Plans are adjusted when they need to be. That ongoing attention is part of what makes care effective, not just the initial diagnosis.
